Acute Respiratory Distress Syndrome (ARDS)
Acute Respiratory Distress Syndrome (ARDS) is a life-threatening condition characterized by acute onset hypoxemia, pulmonary inflammation, and non-cardiogenic pulmonary edema.
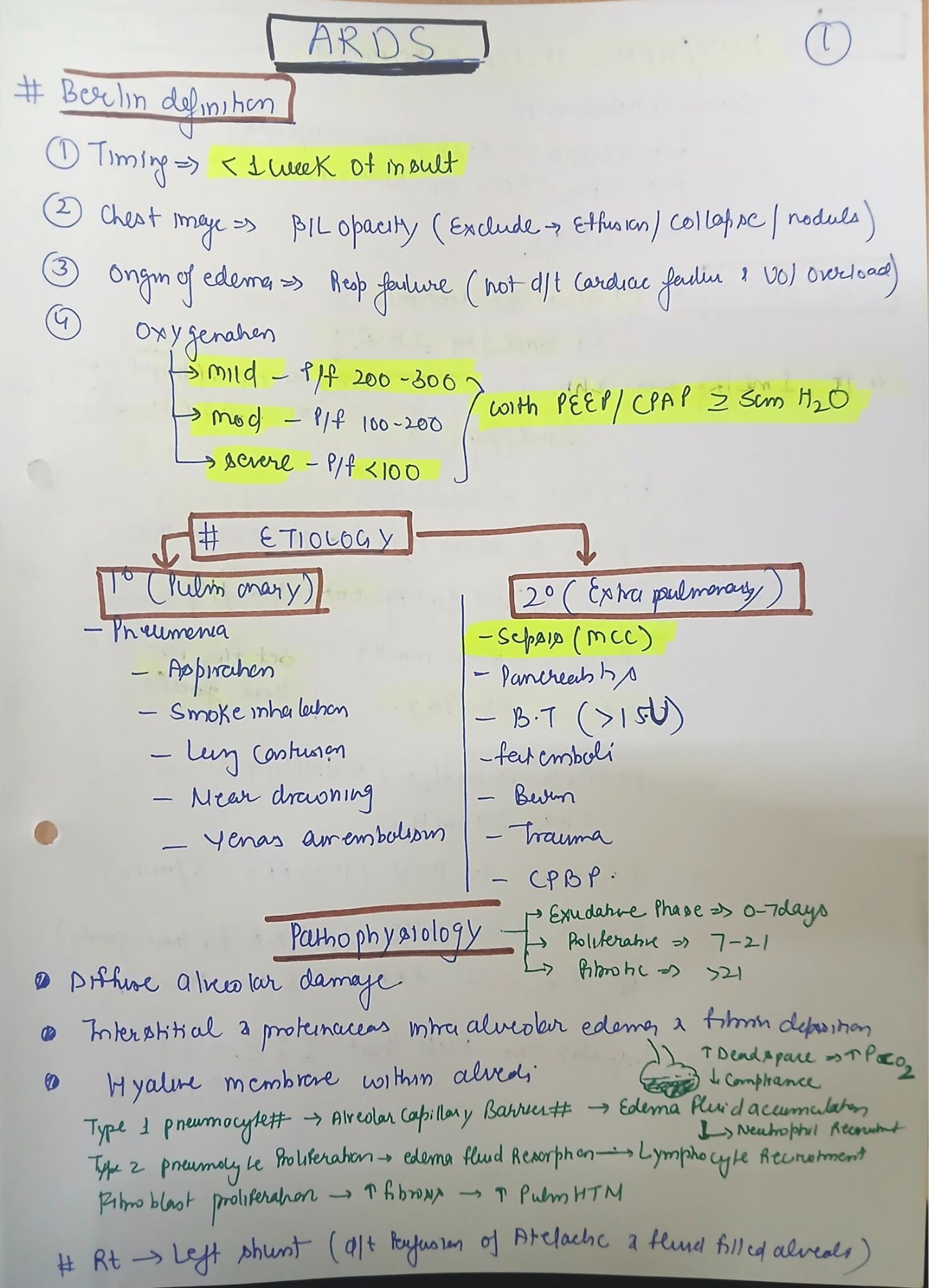
I. Definition & Berlin Criteria for ARDS
Definition:
ARDS is a severe inflammatory lung condition that results in increased pulmonary capillary permeability, diffuse alveolar damage, and impaired gas exchange, leading to severe hypoxemia.
Berlin Definition of ARDS (2012)
To diagnose ARDS, the following criteria must be met:
|
Criteria |
Description |
|
Timing |
Symptoms must develop within 7 days of an insult (sepsis, trauma, aspiration, pneumonia, etc.). |
|
Chest Imaging |
Bilateral opacities on chest X-ray or CT scan, not fully explained by effusions, lung collapse, or nodules. |
|
Origin of Edema |
Not due to cardiac failure or fluid overload (assessed via echocardiography or PCWP <18 mmHg). |
|
Oxygenation Severity (PaO₂/FiO₂ Ratio) |
|
II. Pathophysiology of ARDS
ARDS progresses through three distinct phases:
1. Exudative Phase (Day 1–7)
• Alveolar damage due to cytokine storm (IL-6, IL-1, TNF-α).
• Increased capillary permeability → alveolar flooding → non-cardiogenic pulmonary edema.
• Neutrophil activation → hyaline membrane formation → impaired oxygenation.
2. Proliferative Phase (Day 7–21)
• Alveolar epithelial regeneration begins.
• Macrophages clear debris.
• Fibroblast proliferation → early fibrosis.
3. Fibrotic Phase (>21 days, in severe cases)
• Lung fibrosis leads to chronic respiratory failure.
• Increased dead space ventilation, pulmonary hypertension.
• If severe, progresses to multi-organ dysfunction syndrome (MODS).
III. Etiology & Risk Factors of ARDS
1. Direct Lung Injury Causes:
• Pneumonia (bacterial, viral, fungal, COVID-19 ARDS).
• Aspiration of gastric contents.
• Inhalational injury (toxic fumes, smoke, etc.).
• Pulmonary contusion (trauma).
2. Indirect Lung Injury Causes:
• Sepsis (most common cause of ARDS).
• Pancreatitis.
• Massive blood transfusion (TRALI).
• Trauma, burns, fat embolism.
IV. Clinical Features of ARDS
Symptoms:
• Rapid-onset dyspnea and tachypnea.
• Progressive hypoxemia, cyanosis.
• Decreased lung compliance, increased work of breathing.
Physical Examination:
• Bilateral crackles on auscultation.
• Tachypnea, tachycardia.
• Severe cases: altered mental status, refractory hypoxemia.
Chest X-ray Findings:
• Bilateral diffuse alveolar infiltrates (“white-out lung”).
• No cardiomegaly (to rule out cardiogenic edema).
V. Management of ARDS
1. General Supportive Measures:
• Treat underlying cause (e.g., antibiotics for sepsis, drainage of empyema).
• DVT prophylaxis: LMWH or UFH.
• GI prophylaxis: PPIs or H2 blockers.
• Nutritional support: High-protein, enteral nutrition preferred.
2. Mechanical Ventilation Strategy (Lung Protective Ventilation)
ARDSNet Protocol (Low Tidal Volume Ventilation)
|
Parameter |
Target Value |
|
Tidal Volume (Vt) |
4–6 mL/kg ideal body weight |
|
Plateau Pressure (Pplat) |
<30 cmH₂O |
|
Driving Pressure (Pplat – PEEP) |
<15 cmH₂O |
|
PEEP |
Adjusted per ARDSNet PEEP/FiO₂ table |
|
FiO₂ |
Maintain SpO₂ 88–95%, PaO₂ 55–80 mmHg |
|
Respiratory Rate |
20–30 breaths/min |
|
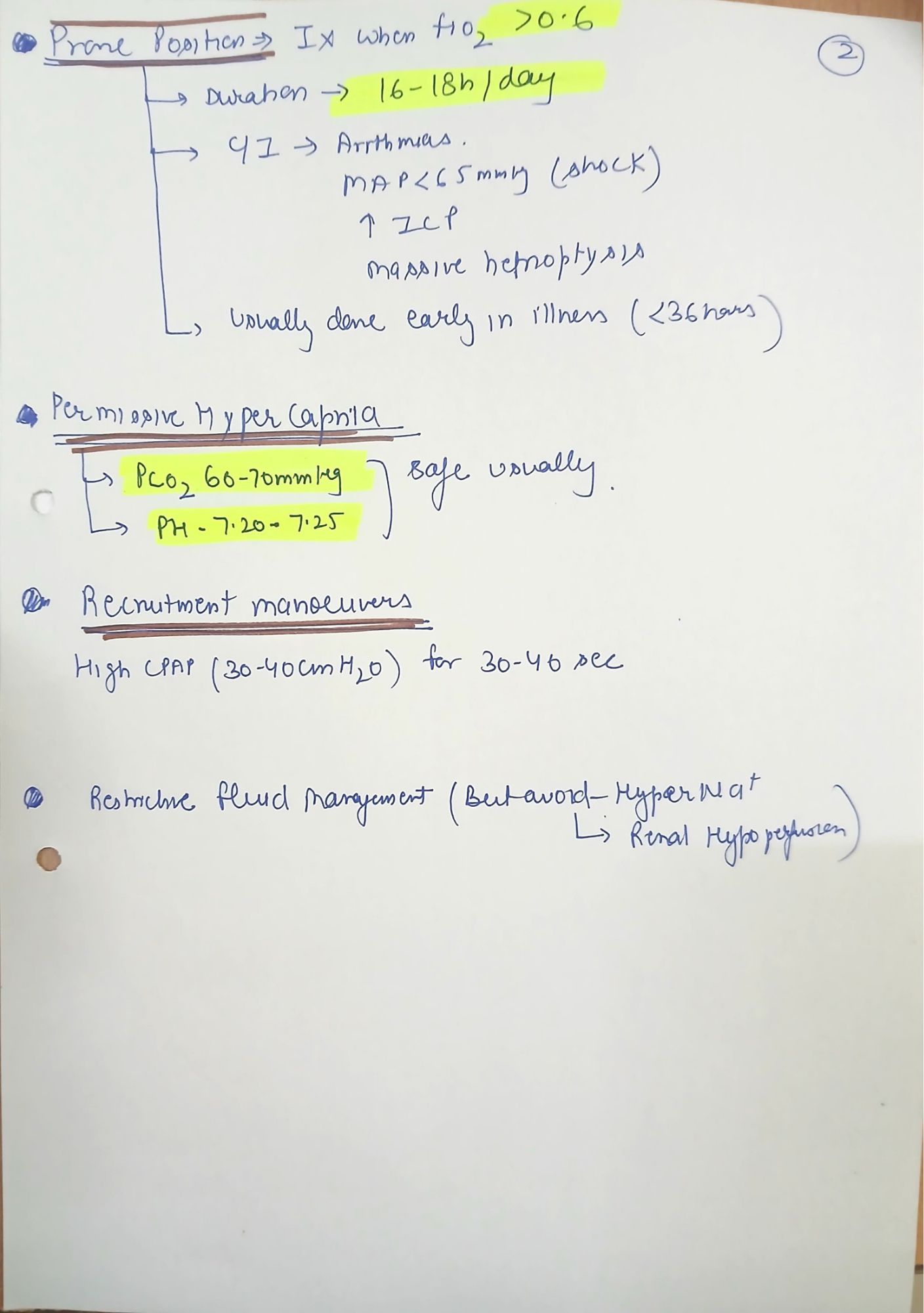
Permissive Hypercapnia |
Allow PaCO₂ up to 60 mmHg if needed |
3. Prone Positioning (For Severe ARDS, PaO₂/FiO₂ <150 mmHg)
• Improves V/Q matching.
• Reduces ventilator-induced lung injury (VILI).
• Recommended for ≥16 hours/day.
4. Neuromuscular Blockade (Cisatracurium)
• Reduces oxygen consumption in severe ARDS.
5. ECMO (Extracorporeal Membrane Oxygenation)
• Indicated in severe, refractory ARDS (PaO₂/FiO₂ <80 despite optimal care).
• Venovenous ECMO preferred.
VI. Recent Updates from Surviving Sepsis Guidelines (2023)
• Prone positioning is recommended for moderate-severe ARDS.
• Higher PEEP strategies should be individualized based on hemodynamics.
• Fluid conservative approach is preferred after initial resuscitation.
• Corticosteroids (dexamethasone 6 mg/day) may be used in COVID-19 ARDS.
MCQs
1. Which of the following is NOT a cause of ARDS?
• A. Pneumonia
• B. Sepsis
• C. Myocardial infarction ✅
• D. Aspiration
2. Which of the following is NOT a feature of ARDS?
• A. Bilateral infiltrates on CXR
• B. Pulmonary artery occlusion pressure >18 mmHg ✅
• C. Severe hypoxemia
• D. Non-cardiogenic pulmonary edema
3. According to ARDSNet protocol, what is the recommended tidal volume setting?
• A. 8–10 mL/kg
• B. 4–6 mL/kg ✅
• C. 10–12 mL/kg
• D. 12–15 mL/kg
4. Which of the following is the most effective intervention for severe ARDS?
• A. High tidal volume ventilation
• B. Prone positioning ✅
• C. Early extubation
• D. Fluid overload